Activity
Mon
Wed
Fri
Sun
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
What is this?
Less
More
Memberships
AI Leverage Society
2 members • Free
Clief Notes
41.1k members • Free
ACQ VANTAGE
1k members • $1,000/month
AI Automation Agency Hub
327.8k members • Free
AndyNoCode
34.8k members • Free
AI Automation Society
418.5k members • Free
28 contributions to AI Automation Society

3d •
Building an AI Operating System for independent pharmacies. Here's the architecture. Tear it apart.
I was a retail pharmacist for 5 years. Independent pharmacies are getting squeezed by PBMs and thin margins, and owners drown in manual work: chasing prior authorizations, re-checking claims for underpayments, calling patients who never picked up. Most of it is repetitive and rules-based, so I automate it. What gets installed: - A Command Center — a local dashboard staff open: today's fills, aged will-call, margin alerts, PA queue. - The AIOS underneath — scheduled automations that ingest the pharmacy's data, run the tools (margin recovery, PA autopilot, patient win-back), and push reports. Nobody has to click anything. The Hardware: Each pharmacy gets a Mac Mini in the back office. I set it up at home, then drop it in. It runs the automations on a schedule and holds all data + dashboards locally, encrypted (FileVault). BestRx is the first pharmacy management system we're working with (Windows-only, can't run on a Mac), so the two machines stay separate. The only thing that crosses is an exported CSV of prescription/claims data: manual export to a watched folder on day one, then BestRx's built-in Scheduled Reports auto-delivers it. BestRx also has an API integration program we're pursuing, so the plan is to move off the manual drag-and-drop CSV entirely and pull the data directly. And before that, if the Playwright CLI can drive BestRx's export screen, we'll try that first to kill the manual step with zero dependency on their side. I run and update every box remotely over Tailscale (WireGuard VPN) — SSH in, deploy a new automation, no site visit. Locked down so only my device reaches any box. Where Claude runs. Claude can't run on the Mini (cloud-only), so I call it through AWS Bedrock under a BAA, billed per token (~$30–150/mo per pharmacy). Two BAAs gate everything: pharmacy↔me, and me↔AWS (so PHI can legally touch Bedrock). The consumer Claude plan is excluded from BAAs, so it never touches patient data. How I stay HIPAA compliant: - PHI stays on the box. The only PHI that leaves goes to Bedrock, legal under the AWS BAA. - Tailscale carries me and my code, never bulk patient files. WireGuard is end-to-end encrypted; Tailscale can't read the stream (the HIPAA "conduit" position). Fallback if needed: self-hosted Headscale. - Human-in-the-loop. The AI reads docs, auto-fills forms, and flags issues. It never submits. A prior auth still needs pharmacist review and prescriber attestation under their NPI. The tool prepares, a licensed human decides. - Claude builds and tests on synthetic data; only fixed, tested code runs on real PHI. No live AI improvising on patient data in production. - Plus audit log, encrypted off-site backups, retention floors.

0 likes • 3d
This is one of the more thought through builds I've seen posted here, the BAA split, synthetic data for building, and the human attestation gate are all the parts people usually skip. So instead of tearing it apart, two things I'd pressure from running production systems for clients. First, the CSV export is your quiet failure point. A watched folder is great until the scheduled export silently stops or the format shifts by a column, and you don't find out until a pharmacist notices missing fills. Put a freshness check on it: if no new file lands by X each morning, you get paged, because "it ran" and "the data is current" are different things. Second, and I say this as someone living it, you are the entire operations team. One Mac Mini per pharmacy that only you can reach over Tailscale means every deploy, fix, and 2am outage routes through you. It scales until it doesn't. Worth thinking now about what happens to a box when you're on a plane, before you have twenty of them. How are you handling a pharmacy that says their numbers looked off last week, can you reconstruct what the system did and when?

3d •
‼️Automated customer bot‼️
I've built an AI chat receptionist, handles customer messages, answers questions, books appointments, the whole thing. Works great on my end. But here's where I'm stuck: when it comes to actually connecting it to a real client's WhatsApp or Instagram account, how does that handoff work in practice? Do you ask them to share API keys? Log into their account for them? Set everything up while they watch? I can't imagine telling a local business owner "send me your Meta Business credentials" and expecting that to go smoothly. How are you guys handling this? Is there a clean way to onboard a client without it turning into a security nightmare or a trust issue?
0 likes • 3d
You've already got the right instinct, if it feels wrong to ask for their password it's because it is. The clean version: you never hold their credentials and you never log in as them. Every real platform has a delegated access path built for exactly this. On Meta you have them add your business as a partner from their Meta Business Suite settings (their business portfolio), using your business ID, and grant scoped access per asset. They click approve inside their own login, and they can revoke it any time without touching a password. For WhatsApp the number and the WhatsApp Business Account stay owned by them, you just get permissioned access to send and receive through the Business Platform, no raw login handed over. When I onboard a client I walk them through granting on their side while we're on a call, so they watch access get handed over and see that it's revocable. That framing is what kills the trust worry, they're not giving you keys, they're granting a permission they control. Are you on the WhatsApp Business API or automating the regular app? The onboarding path is pretty different depending on which.

3d •
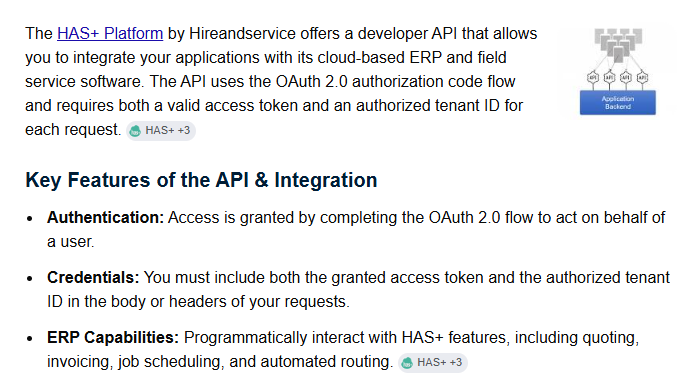
API Integration
I am planning/started developing using Claude Code. Fairly simple: The user will log onto the app I am developing, view data on a Supabase database, update and save. So far, everything is easy. Help needed:- Only the data fields to be edited will be pulled from an existing database of a web CRM system, and once the data is edited by the user using the app, the updated data must be pushed back to the CRM database again. In priciple I understand what an API must do and, at a high level, how it works, but since I have never done an API Post and Call (I am not a developer), I would like to know what I need from the developers of the CRM system If someone has a playbook info for me I can follow for that integration, I would really appreciate some help/pointers This is all I have for now, hence I would like to know what else, if I need, I should ask for: https://www.hireandservice.com/terms/developer
0 likes • 3d
Since you're not a developer, the useful move is to ask the CRM team for a short specific list so you're not stuck decoding docs. What you actually need from them: the base URL for their API, how auth works (API key, OAuth, something else) and how you get a key, the exact endpoints to read the fields you want and to write them back, the field names and types for those, whether there's a rate limit, and whether they have a sandbox or test account so you're not editing live client data while you learn. One more that saves pain later: ask whether a write creates or updates in one call, or whether create and update are separate calls, because pushing edited data back is where people accidentally make duplicates. If they can hand you one example request and response for a read and for a write, Claude Code can usually take it from there. Is the CRM a known one with public API docs, or fully custom? If custom, that list is exactly what unblocks you.
5d •
Solo builders: how did you actually take yourself out of the critical path?
Honest question for the solo operators here, because I don't have a clean answer. What makes a solo operation fragile isn't the building, it's that I am the bottleneck on everything that matters. Every deliverable, every fix, every judgment call routes through me. That caps how much I can take on, and nothing ships when I step away. The obvious answer is delegate, to people or to agents. The part nobody tells you is that quality usually drops the moment you hand something off, so you end up redoing it, which is slower than just doing it yourself. So you pull it back, and you're the bottleneck again. What I've tried so far: writing the boring repeatable parts down as steps, handing off the pieces where wrong is cheap and easy to catch, and keeping a human gate on anything client facing. It helps at the edges, but I'm still the single point of failure on the core work. So the real question for anyone who's actually done it: how did you take yourself out of the critical path without the quality dropping? Was it better SOPs, hiring a specific role first, leaning on agents for a slice of it, something else? What was the first thing you successfully stopped doing yourself?
0 likes • 5d
@Ahmad Khan Documenting the decision making over the steps is the direction I'm circling too, the steps were never really the bottleneck, the judgment was. To your question, the piece I still can't hand off is the final client facing review, the "is this good enough to send" call. Mechanical stuff I've managed to write down, but taste on a deliverable I keep failing to put into words, so it stays with me. Have you found a way to encode that kind of judgment, or does it just stay with the owner? That's the part I'm trying to crack.
0 likes • 3d
@Ahmad Khan Yeah, and I think you're onto the thing I kept missing. I tried to write taste down as rules and it never survived contact, the good deliverables just have too much "you'll know it when you see it" in them. Examples carry that better than any rule I can write. The one thing I'd add from trying it: the pair only teaches if you label WHY each one is approved or needs work, otherwise the model (or the person) pattern matches on the wrong feature, like copying the format instead of the judgment. So it's less a folder of good and bad, more a folder of good and bad with a one line reason attached. Have you found the reason matters as much, or does the raw example carry enough on its own?
6d •
How are you checking your agent's output is still good, not just that it ran?
Something I keep hitting and don't have a clean answer for. Catching when an automation BREAKS is easy. It errors, nothing comes out, you get an alert. Catching when it quietly gets WORSE is the hard one. The thing runs fine, returns something that looks right, but the quality slipped and nobody notices for two weeks. For the mechanical parts (did the row get created, did the email send) this is simple. For anything open ended (a draft, a summary, a reply, a piece of content) I have no clean way to score it automatically. "It produced text" is not the same as "it produced good text." What I do now is a mix: a few hard checks on the mechanical parts, a human spot checking a sample, and saving the bad outputs so I can see patterns. It works, but it's manual and it doesn't scale past a handful of automations. So the open question for people running this in production: how are you measuring whether an agent's output is actually good over time, not just that it ran? Anyone using a model to grade another model's output, and does that actually catch the slips or does it just rubber stamp them? Curious what's working.
0 likes • 3d
@Mike Donk Fair, and you've moved me here. I was still framing drift as something to eliminate, and you're right that you can't. The inputs and the world keep moving, so the target never holds still. So the honest answer to "how would I know I designed it out" is I wouldn't, and chasing that certainty is the wrong goal. Managing it means the measurement never turns off, it just gets cheaper to run. Where do you draw the line on how tight to manage it? I assume not every automation earns the same rigor, so how do you decide which ones get the heavy monitoring and which you let run looser?
0 likes • 3d
@Dionny Chejito That's the cleanest fix I've heard for it. Fixed set for the trend line, one rotating wildcard from live traffic for the drift signal, so you get comparability and freshness without polluting either. I was treating it as one or the other and you just split them. Stealing this. Quick one: does the wildcard ever get promoted into the permanent set if it exposes a failure mode you want to keep watching, or does it always rotate out?
1-10 of 28

@thanh-dinh-4764
Founder, Spectral Point AI. I build AI systems for program creators and businesses, in production not demos. I run AI Leverage Society here.
Active 1d ago
Joined Jul 18, 2025
Springfield, Missouri
Powered by