Activity
Mon
Wed
Fri
Sun
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
What is this?
Less
More
Owned by Nabila
Cardiology education & community for medical students, nurses, PAs & doctors – clear, practical, career-focused.
Memberships
27 contributions to The Cardiology Tutor
23d •
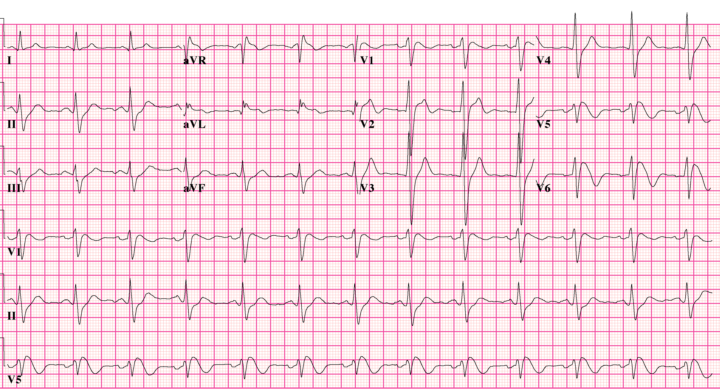
This ECG got a completely healthy 23-year-old banned from competitive sport. Why?
Question: What is the MOST likely diagnosis? Answer revealed tomorrow but I want to see your answer and reasoning. Good luck!🤞
Poll
3 members have voted
0 likes • 21d
🚨 ANSWER REVEALED 🚨 The diagnosis is: ✅ Brugada Syndrome Type 1 This ECG is considered diagnostic. Key clue #1 Don’t focus on the QRS. Focus on V1-V3. Key clue #2 Notice the: - Coved ST elevation - Downsloping ST segment - T-wave inversion This is the classic Type 1 Brugada pattern. Why was the athlete banned? Because Brugada Syndrome is associated with: ⚠️ Ventricular fibrillation ⚠️ Sudden cardiac death ⚠️ Syncope ⚠️ Nocturnal arrhythmias Many patients are completely healthy until their first arrhythmic event. Teaching Pearl The most dangerous ECGs are often not the ugliest. This patient could have: - Normal echocardiogram - Normal exercise capacity - No symptoms Yet still be at risk of sudden cardiac death. That’s why recognising Brugada matters.
23d •
We are back and huge announcement!
Good morning team, hope you’re well? We will be announcing new course dates on here very soon, you will be first to know. Otherwise how are you all and let me know if you have any questions.
1 like • 23d
@Ifza Zia fantastic. Well I respect your patience and stay tuned becuase all details will be released very soon ☺️
Nov '25 •
Catch up
Quick one guys- would you like to have a quick LIVE call next week? Ask me anything related to career, clinical, medical etc
0
0
Oct '25 •
Handheld Echocardiography Course
Next course date out. Please DM for those who want to apply.
0
0
Oct '25 •
📣 3 Days to Go – The UK Medical Student Survival Guide 🚀
Hi everyone 👋 We’re just 3 days away from the release of The UK Medical Student Survival Guide 🎯 This guide has been built from real experience — everything I wish I’d known as a medical student, distilled into practical frameworks you can actually use on the wards and in exams. ✅ OSCE and presentation templates ✅ ECG and cardiology shortcuts ✅ Study structure + placement mindset ✅ Consultant-level clinical tips It’s not just another textbook — it’s a real-world survival manual written by someone who’s been through it all. 💬 Action: If you’ve found this community helpful, pass it on to your peers and colleagues — medical students, FY doctors, or anyone who’d benefit. Tell them to join this Skool group now so they don’t miss the launch on Monday. Trust me — this one’s not to be missed. 👇 (You can also drop in the comments where you’re studying or working — I’ll give a shoutout to a few of you in the launch post!)
0
0
1-10 of 27
@nabila-laskar-6144
Cardiology education & community for medical students, nurses, PAs & doctors – clear, practical, career-focused. only with Dr Nabila Laskar
Active 1d ago
Joined Sep 11, 2025
London