Activity
Mon
Wed
Fri
Sun
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
What is this?
Less
More
Memberships
Tony Huge Evolution
3.9k members • Free
The Iron Forge Brotherhood
25.1k members • Free
3 contributions to Tony Huge Evolution
Mar 17 •
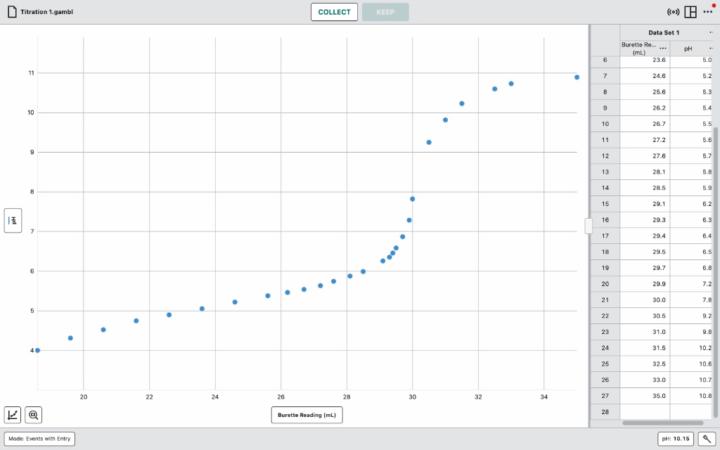
8-week IGF-1 LR3 cycle
Hey all, I’m putting together a plan for an IGF-1 LR3 run and wanted to get some experienced opinions, specifically around cycle length. I know the standard protocol is 4-6 weeks due to receptor desensitization . However, my situation is a bit specific, and I’m trying to figure out if the standard advice applies the same way to me. My Situation: · I have 2mg total of IGF-1 LR3 to work with. · My plan is an 8-week cycle, tapering the dose to make the supply last (e.g., 30/35/40/40/40/40/30/30 mcg/day or similar). · I will not run IGF-1 LR3 again for a very long time (at least a year or two) after this. Receptor resensitization for a future cycle is not a concern for me. · About a month after finishing the IGF-1 LR3, I plan to hop back on Retatrutide. I’m also on 25 mg Mk677 right before sleepjng My Understanding (and Questions): 1. Receptor Desensitization: My primary research tells me this is the main reason for short cycles . Since I'm treating this as a one-and-done blast, is receptor sensitivity still a critical factor? Or does the risk of diminished returns in the final weeks outweigh the benefit of running it longer? 2. Are there other risks with a longer cycle? Besides getting used to it, what other potential downsides should I be aware of with an 8-week run? · Hypoglycemia & Insulin Resistance: I know LR3 has a ~20-30 hour half-life and impacts glucose uptake . Does the risk of developing insulin resistance increase significantly after 6 weeks? · Mitogenic/Cellular Growth Concerns: I've read about the theoretical risks of IGF-1 promoting cell proliferation and its link to cancer pathways . Is an extra 2-4 weeks of exposure in a single cycle a meaningful increase in this theoretical long-term risk? · Systemic Stress: Will running it for 8 weeks put more strain on things like appetite, digestion, or cause other systemic sides that typically ramp up after a month? I get that more isn't always better, but I’m trying to balance making the most of the supply I have with not being stupid about it. If the only real downside of an 8-week cycle is that I might get slightly diminished returns in week 7-8, I can live with that. But if I'm significantly increasing my risk of insulin sensitivity issues or other long-term problems, then I'll stick to the 4-week protocol.
Jan 28 •
CNS Fatigue
Are there any peptides out there or anything specifically for CNS fatigue? I was told about cerebrolysin but I am not comfortable injecting 5 ml of something into me everyday. I want something that accelerates recovery of CNS.
Jan 21 •
Stack questions
Stats & Goal: · Male, 20, 182 lbs · Cutting to 168 lbs. · Current BF: ~24% · Lifting: Currently following a PowerBuilding program. The Core Cut Stack: 1. Retatrutide: 2mg/week. Titrated slowly, pre-medicated. 2. YK-11: 15mg IM twice weekly (MCT oil, pinned Sun/Wed). 3. Enclomiphene: 6.25mg daily (SERM base). 4. MK-677: 25mg nightly. 5. Cardarine: 20mg daily (AM, SUBQ) [In transit]. 6. DMAA Pre: Used sparingly. Supplements: · Liver: TUDCA 500mg + NAC 600mg daily. · Electrolytes: Comprehensive protocol. · General: Fish Oil, Vitamin D, etc. · Sleep (Adding Soon): DSIP (150mcg nightly), Epitalon (10mg/day pulse). Diet: ~500 cal deficit, 220g+ protein, 65g fats. --- My Three Key Questions: 1. Is my YK-11 dosing and schedule optimal? * Dose: 15mg IM twice weekly (30mg/week total). * Rationale: Balancing myostatin inhibition for muscle retention against sides. Also that’s what a jailbroken AI told me to take 2. What critical support compounds am I missing? Fighting significant fatigue. * Deep systemic fatigue is the main battle. DMAA helps in-gym only. * Considering: SS-31 or MOTS-c for mitochondrial energy. Cost is high though and can’t afford 3. How should I structure training intensity? (Most urgent question) * AI/fitness consensus often recommends RPE 7-8 on a cut to manage fatigue. * However, my stack (YK-11 for myostatin inhibition, MK-677 for recovery) provides anti-catabolic protection. * My Hypothesis: I should train higher intensity (RPE 9-9.5) on primary compound lifts to provide the maximal "keep this muscle" stimulus, while drastically reducing back-off volume to manage systemic fatigue. Then keep accessories in the 7-8 range. * Is this right? Or is sticking to the conservative 7-8 RPE across the board smarter, letting the compounds do the preservation work? Context: The goal is maximum muscle retention. The fatigue is real, but I can push through focused, high-intensity sessions. I need to know if pushing the RPE is a strategic advantage or a recoverable fucking mistake.
0 likes • Jan 23
@Dan Hybrid gotcha, thank you so much for the advice!
1 like • Jan 23
@Aaron Reed what dose would you split it into?
1-3 of 3